Materials and Methods
2.1. Study Design
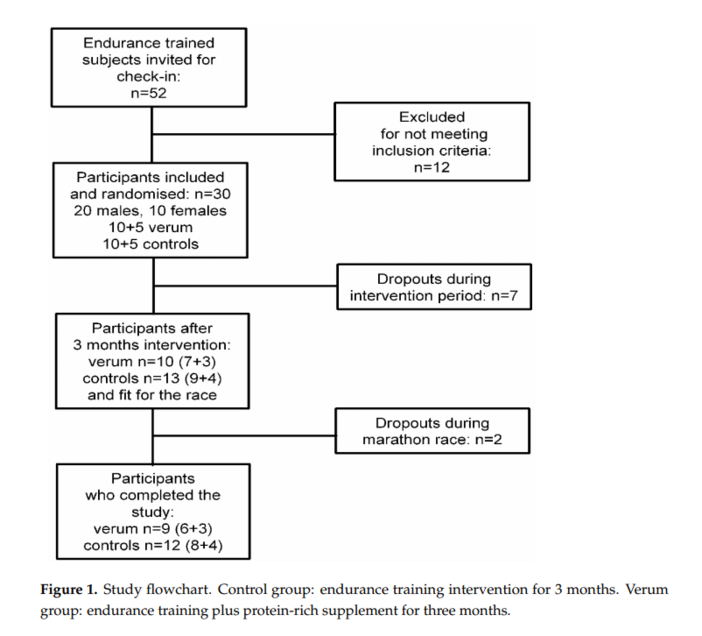
The study was designed as an experimental RCT to determine the effects of a protein-rich supplementation regime across a 3-month training period on the endurance performance and training adaptation, ultimately evaluated with a marathon race at the end of the intervention compared to a control group. Participants study visits were conducted at baseline (termed “a”) and at the end of the 3-month training intervention (termed “b”) as well as before (termed “c”) and 1 h after (termed “d”) the marathon race at the end of intervention. The period between visits “b” and “c” lasted approximately 7 days, but the athletes had to continue with the protein supplementation regimen until the marathon race day. After the “a" visit, study participants were randomly assigned either to the intervention or control group.
2.2. Participants
After contacting and advertising the study protocol to regional sports clubs, 30 out of 52 applicants met the criteria for randomisation (defined as experienced endurance runners) to either a verum (V; n = 15, 10 males, 5 females) or a control group (C; n = 15, 10 males, 5 females). Participants had to fulfil the following inclusion criteria: to be clinically healthy endurance-trained adults, aged between 18–60 years, and a body mass index (BMI) between 18–25 kg/m2. Additional inclusion criteria were: constant roadwork training (ca. 3 times per week of 25–30 km endurance training), non-use of other nutritional or ergogenic supplements, no blood lipid- or glucose-lowering therapy within the preceding 12 months, being non-smoker, alcohol consumption <40 g/d, and a relative maximal oxygen consumption (VO2max) between 45–65 mL/kg/min. The study protocol was registered and approved by the Ethical Commission of the University of Freiburg (reg. no. 231/12). The study was conducted in accordance with the ethical standards established in the 1964 Declaration of Helsinki and its later amendments [12]. All participants were informed verbally and supported by a written participant information sheet, and signed consent to participate in the study was obtained.
2.3. Protein Supplementation
The supplement used (comparable with the commercially available product Almased-Vitalkost®; Almased-Wellness-GmbH, Bienenbüttel, Germany) is composed of soy protein, skimmed milk powder, and honey without additives. The protein content of this product is 53.3% (83% soy-protein-isolate, and 17% milk protein). Given the special marathon conditions, each 50 g portion was supplemented with 9 g palatinose, 30 mg carnitine, 10 mg coenzyme Q10, and 0.5 mg α-lipoic acid. One portion thereby equated to 60 g of powder dissolved in 300 mL water, providing 217 kcal, 27.2 g protein, 24.6 g CHO, and 1.0 g fat. Participants were instructed to drink one portion twice per day, in the morning before breakfast and in the afternoon or evening, with each intake always approximately at the same time of day and with a delay before ingestion of other meals to account for the low glycaemic load of the product.
2.4. Measures
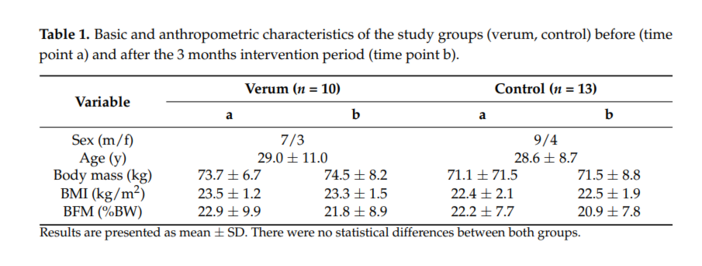
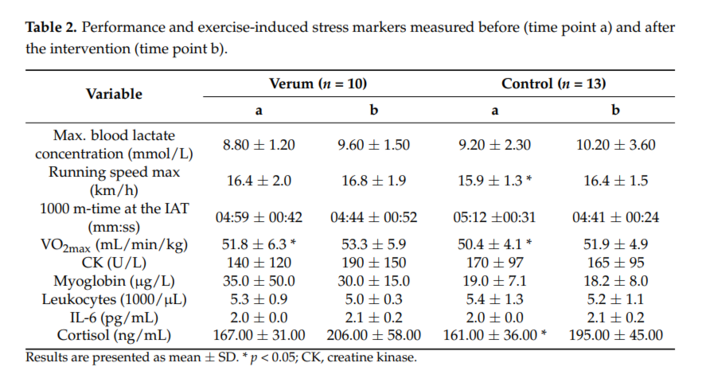
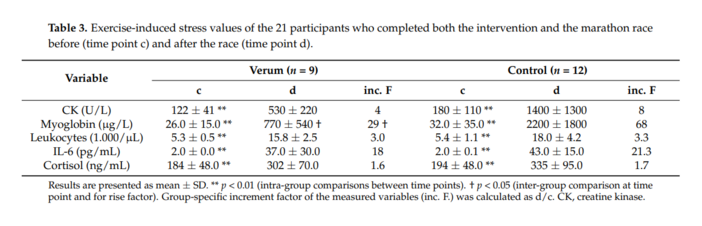
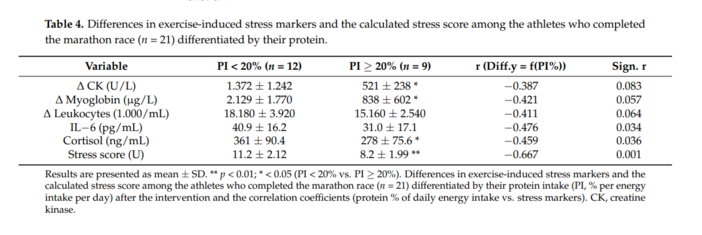
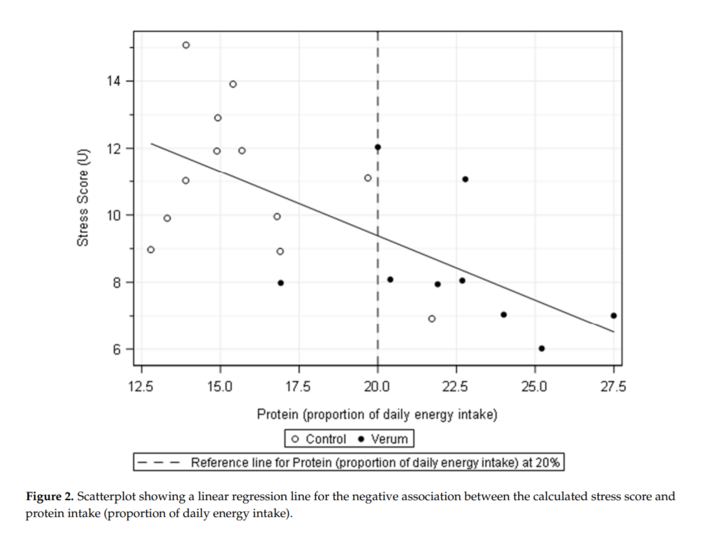
The participants’ accordance with the inclusion criteria was confirmed in the initial comprehensive health screening before the intervention. Laboratory analysis of blood samples as well as the measurement of anthropometric parameters were concomitantly performed. Anthropometry comprised body height (BH), body mass (BM), and body mass index (BMI). BM was measured in light clothing to the nearest 0.1 kg, BH to the nearest 0.5 cm (Seca Stadiometer 274, Seca GmbH & Co. KG, Hamburg, Germany), and BMI was calculated with the formula: weight in kilogram divided by height in meters squared. Percentage body fat (FM%) was calculated using the Siri equation [13] with the log sum of skinfold thickness (SFT) at 4 measuring sides (triceps, biceps, subscapular, and suprailia). The SFT was measured using a skinfold calliper (Lange Skinfold Caliper, Beta Technology Inc., Noblesville, IN, USA). The laboratory analyses included selected metabolic variables for performance diagnostics (blood lactate concentration [14]), whole blood cell counts (including leukocytes [15]), selected blood indicators of muscle damage and systemic stress (creatine kinase (CK) [16], myoglobin [17] and interleukin-6 (IL-6) [18]), and the hormone cortisol [19]. Biochemical blood variables were determined by venous blood sampling. Leukocyte count, cortisol, and indicators of muscle damage and stress response were utilised in the calculation of a “stress score” (unpublished “in-house” method to determine overall exercise-induced stress response), which was expected to be noticeably increased after bouts of hard endurance exercise, such as a marathon race. For this purpose, the participants’ values for each of the variables were ranked in ascending order and categorised into three equally sized groups. For each parameter, the participants were assigned to one of the three categories, reaching a stress score of 1 for a relatively low parameter increase, 2 for a moderate increase, and 3 for a high increase. Hence, for each participant, a final total stress score was calculated ranging from a possible minimum of 5, showing low levels for all 5 variables, to a maximum score of 15. Mean stress scores were calculated for both study groups. The comprehensive health screening also included performance diagnostics to assess the training status of the participants and were conducted as a treadmill test using spiroergometric equipment (ZAN Messgeräte GmbH, Oberthulba, Germany) following the ZAN protocol of sequential 3 min steps with increasing running speed [14,20]. After each increment to the maximal possible load (running speed max), a capillary blood sample was taken from the earlobe for blood lactate concentration measurement as well as immediately after the termination of the test to obtain the maximal blood lactate concentration. These lactate values were used to calculate the individual anaerobic threshold (IAT) [21]. The running speeds at the described thresholds were transformed into the theoretical time needed individually to reach 1000 m (1000 m time at the IAT). Participants were tested 3 h after breakfast. Blood samples were also drawn prior to performance diagnostics. In addition, the participants were requested to avoid highly intensive physical activity and strength exercise on the previous day to prevent post-training alterations in the pre-test blood samples acquired.
2.5. Training Phase
To estimate training compliance and comparability of training volume and exercise intensity between the groups, the participants were requested to complete training protocols, documenting weekly training distances and training time over the 12-week intervention phase. The entire training phase was supervised by experienced endurance trainers in both groups. Furthermore, participants were requested to complete a 3-day estimated nutrition protocol before and after the intervention period and were advised to maintain their typical eating and drinking patterns. The evaluation of the food records was performed using the EBISpro nutrition system (Stuttgart, Germany) [22].
2.6. Statistics
Prior to analysis, data were checked for normality distribution. Intragroup comparisons between baseline and post-intervention as well as before and after the marathon race were assessed by the Wilcoxon signed-rank test. Intergroup comparisons were analysed by the Mann–Whitney U test. Spearman’s rank correlation analysis was performed to determine the influence of macronutrient intake on muscle stress reactions. The variables “Diff. Myoglobin (µg/L)” and “Diff. CK (U/L)” were log transformed due to variance inhomogeneity and the analyses (correlation, regression analysis and t-test) were conducted with the transformed variables. SPSS 22.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. All statistical tests were two-sided, and the level of significance was set at α = 0.05.