Discussion
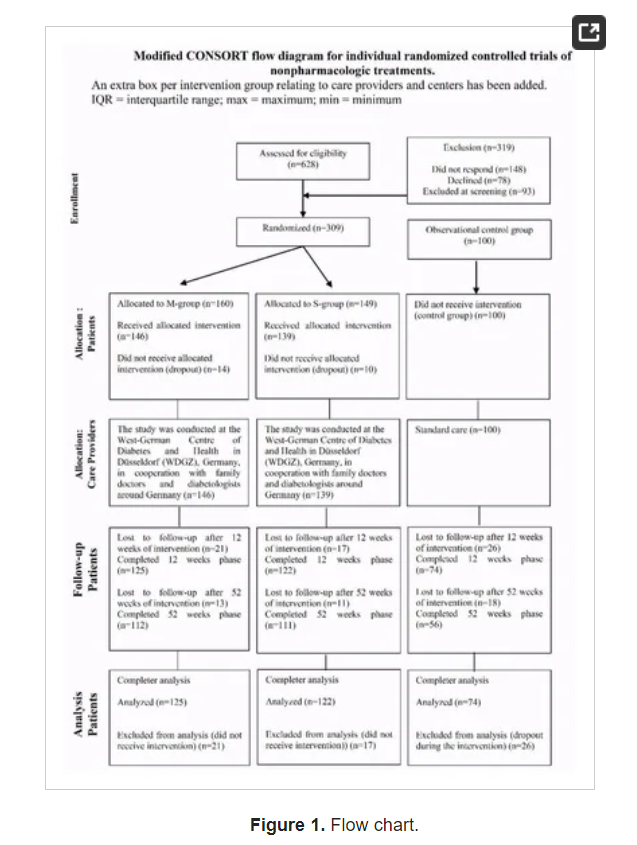
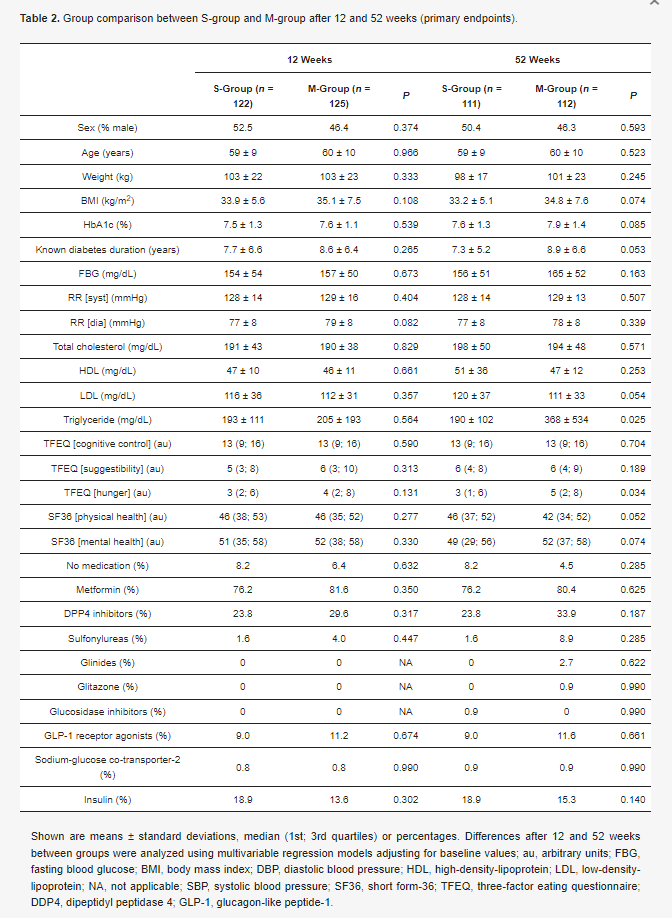
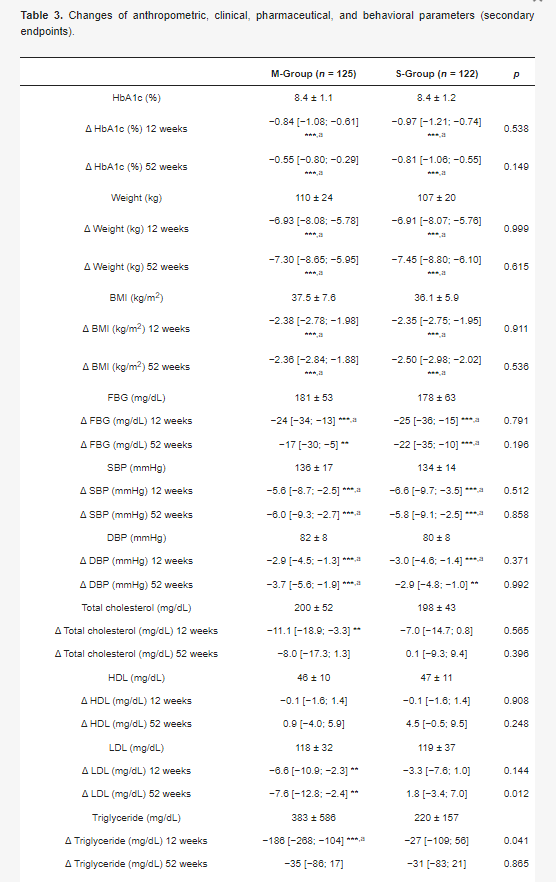
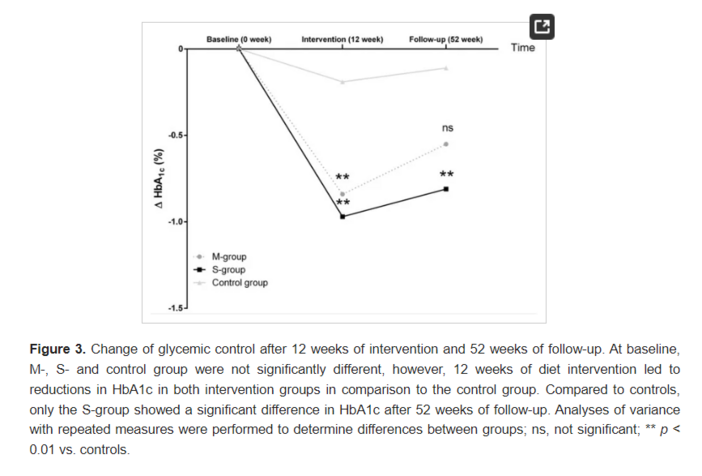
The results of the present study demonstrate that an individualized meal replacement therapy starting with intense low-carbohydrate formula diets and SMBG-accompanied reintervention of low-carbohydrate meals lead to clinically relevant improvements in HbA1c after 12 weeks of intervention in patients with poorly controlled long-standing type 2 diabetes. Particularly, patients of the more intense intervention group (S-group) showed long-term clinically relevant improvements after 52 weeks of follow-up as compared to the participants of the moderate intervention group (M-group), although this difference was not statistically significant. Furthermore, the overall dropout rate after allocation into both intervention groups was small (247:285; 13%) and not different (S-group = 12% and M-group = 14%). We hypothesize that the strict rules, the stringent and individual SMBG [17], and the complete replacement of all meals in the S-group during the first week contributed to a subtler change of behavior and higher motivation for the diet, which was shown to be necessary for long-term changes of behavior in high-risk individuals for type 2 diabetes in prior studies [19]. Furthermore, we assume that our personalized nutrition and treatment-approach with a more intense patient empowerment during the first week in the S-group contributed to a long-term difference in HbA1c after 52 weeks of follow-up. The recently published DIRECT study has demonstrated that a strict calorie restriction with only 825–853 kcal per day for 3–5 months contributes to significant improvements of HbA1c (−0.9%) and body weight, and in the further course to diabetes remission after 52 weeks of intervention [13]. However, the formula diet contained proteins and carbohydrates in a ratio of 1:2 [13]. We chose an opposite formula diet that was high in protein, but low in carbohydrates (ratio nearly 2:1) with individualized moderate-calorie supply (1300–1500 kcal/day), because we postulate that a higher amount of carbohydrates would stimulate an increase in insulin release and a decrease in fat burning [20]. Therefore, our strong carbohydrate reduction with an accompanied stepped food reintroduction should lead to long-term benefits like it was shown before in the DIRECT study [13]. Another explanation could be that the S-group was somewhat higher motivated to be physically active due to the complete change of nutrition and behavior, respectively. Previous studies have already demonstrated strong effects on HbA1c through very low-calorie liquid formula diets in small groups of patients with type 2 diabetes (n < 30) during an investigation period up to 26 weeks, especially after a short duration of diabetes (<4 years) [11,14,15]. This correlation between diabetes duration and changes of HbA1c after 12 or 52 weeks could be confirmed in our study by the whole intervention cohort (r = 0.226 (after 12 weeks) or 0.229 (after 52 weeks); both p < 0.001), independently of age.
Our approach of low-carbohydrate meal replacement is based on the recommendations for diets in type 2 diabetes, as well as recently published reviews and meta-analyses [21,22]. Although, a healthy diet is crucial for type 2 diabetes, there still exists controversy in the field about the feasibility and mechanisms of these stringent types of dietary interventions and their long-term effects in HbA1c [23]. The effects on the glucose metabolism (e.g., anti-diabetic medication was adjusted within the first week) occur immediately after beginning the meal replacement therapy [12] and before a significant weight loss takes place. The observed effects are comparable with those after bariatric surgery [7]. Possible explanation approaches in this context could be altered levels of incretin secretion [24], improved mitochondrial oxidative function [25], energy restriction [10], the sudden negative energy balance [14], or a combination of all these points. Furthermore, a reduced carbohydrate intake [26] or a reduced number of carbohydrate-containing meals might trigger the fast effects on the glucose metabolism. This would be in line with observations that two meals per day are better than six [27] for type 2 diabetes patients, especially in terms of body weight, insulin resistance/sensitivity, and beta cell function [10]. The results of the PREDIMED study, in which two high-fat/lower-carbohydrate Mediterranean diets were compared to a fat-reduced diet regarding the incidence of type 2 diabetes [28] or cardiovascular events [29], as well as changes of body weight and waist circumference [30], support our findings that carbohydrate-reduced diets are beneficial for patients with type 2 diabetes.
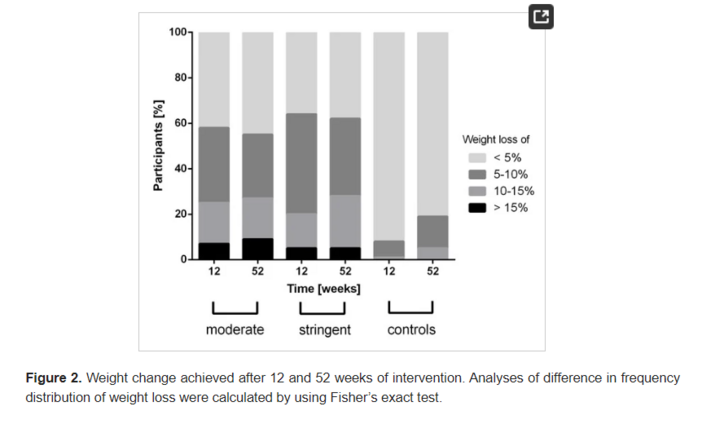
The improvements in glycemic control in both intervention groups in the present study were followed by strong reductions in body weight (Figure 2). In a recently published meta-analysis, it was shown that very low-calorie (<800 kcal per day) or low-energy liquid-formula (>800 kcal per day) diets can induce large reductions of body weight (ranging from 8.9 to 15.0 kg) in obese people (BMI: 35.5–42.6 kg/m2) with and without type 2 diabetes [31]. The slight difference in body weight reduction in our trial can be explained by a higher calorie consumption per day (≈1300–1500 kcal per day) when compared to the studies of the meta-analysis. Furthermore, our results are comparable to the findings of Steven et al. [11], who works with a very low-calorie and moderate-carbohydrate composition (43% carbohydrate, 34% protein, and 19.5% fat; 2.6 MJ/day [624 kcal/day]). They found that a very low-calorie diet over eight weeks can contribute to a meaningful weight reduction of ≈14 kg, which was still comparably high, even after 26 weeks (≈13 kg) in individuals with type 2 diabetes. In regard to the aforementioned findings, we could demonstrate similar results of weight reduction with ≈7 kg after 12 and 52 weeks of intervention. In contrast to Steven et al., we designed an individualized low-carbohydrate and moderate-calorie diet intervention (31% carbohydrate), accompanied with SMBG as it might be more feasible for patients with type 2 diabetes, characterized with eating and motivation impairments [32]. The improvements, apart from the meal restriction, could be therefore also explained by improved education regarding nutrition, physical activity, and blood glucose control.
A recently published review supports our approach, as it states that a rather moderate weight loss is more sufficient for the transition from metabolically unhealthy obesity to metabolically healthy obesity with a lower risk for adverse outcomes in the long run than a large amount of weight loss in a short period [33]. We chose this calorie goal per day in order to reduce the rate for dropouts and increase the participants therapy adherence. Lifestyle interventions are always criticized in terms of their long-term effectiveness, and one possible hypothesis says that the major problem is that patients fail to adhere to the altered lifestyle prescriptions [34]. In contrast to many other long-term lifestyle intervention programs [35], the relatively high number of completers after 12 (83%) and 52 (72%) weeks supports our study design and approach. Potential reasons for nonadherence comprise: age, perception and duration of disease, polytherapy, social and psychological factors, costs, dislike for foods included in meal plans, education and a lack of understanding of the long-term benefits of treatment, adverse outcomes (e.g., weight gain or hypoglycemia), as well as negative treatment perceptions [36]. In this context, new innovative methods are needed to assist those patients. In light of these problems, we designed the study with almost no barriers for the participants (e.g., 1:1 personal support or no additional costs) and provided every participant with a personalized meal replacement and supported them in their SMBG.
Further improvements were achieved in the cardiometabolic parameters of fasting blood glucose, as well as systolic and diastolic blood pressure. These results are confirmative regarding other studies with low-calorie diets in patients with a short- and long-duration type 2 diabetes and moderate [14] or poor glycemic control [10,15]. Our results are also confirmed by a recently published review in terms of improvements of the cardiovascular risk profile in patients with type 2 diabetes showing a significant decrease in systolic and diastolic blood pressure as well as fasting blood glucose after low-calorie diets [37].
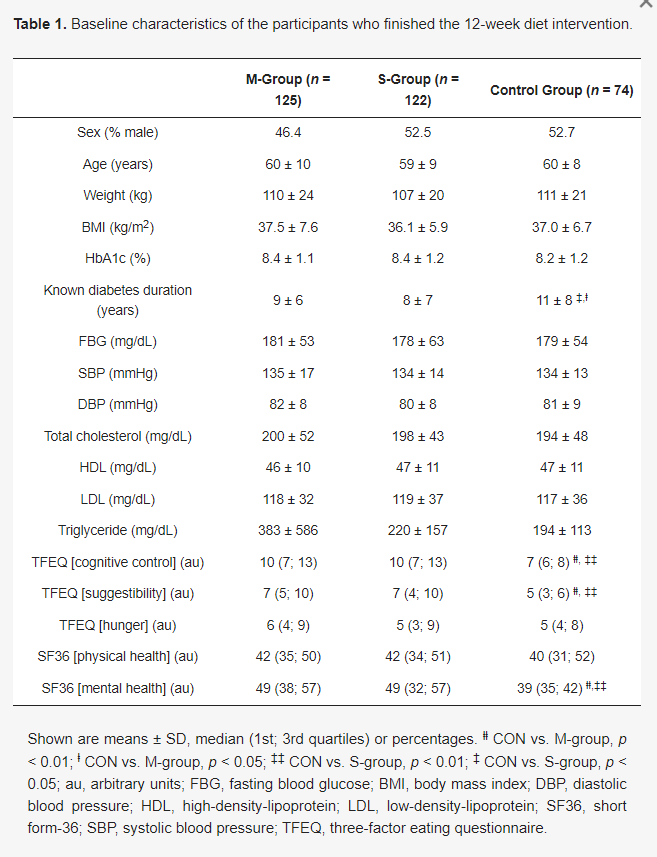
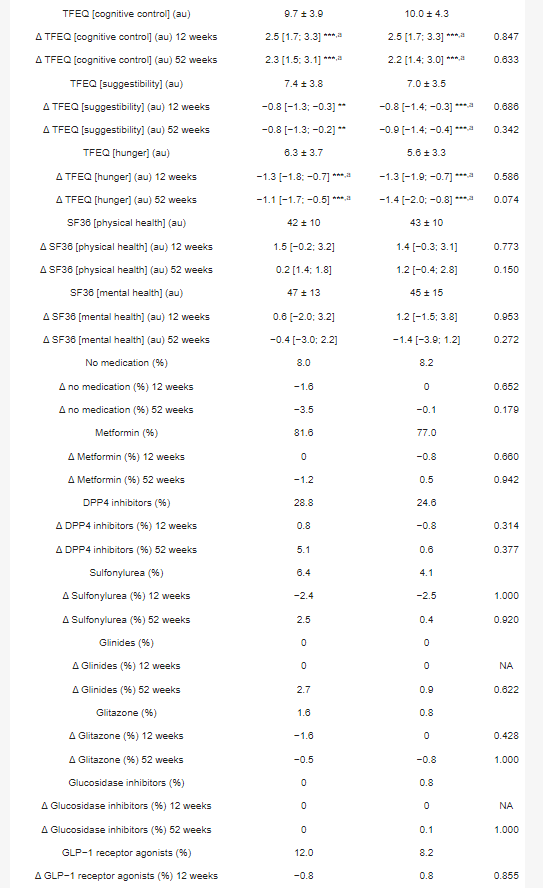
A further positive effect following the intervention was the improvement of eating behavior in the intervention groups. The simple and structured formula diet reduced feelings of hunger and increased the control regarding eating-associated actions. In patients with type 2 diabetes, a disordered eating behavior can be present and it is associated with poor quality of life [38]. When compared to individuals with the metabolic syndrome, type 2 diabetes participants of the present intervention groups showed a pronounced feeling of hunger and a weaker control over their suggestibility for food [39]. Another study supports our findings showing meaningful improvements in eating behavior after a three-month mindful eating intervention in non-insulin requiring patients with type 2 diabetes in a small cohort (n < 30) [40].
A previously published pilot study [12] revealed how a formula diet affects blood glucose control and weight, and how insulin is reduced or discontinued. However, it was also shown that participants sometimes found it difficult to maintain the stringent diet during the first week. Therefore, we were interested in whether a moderate approach also leads to success. The underlying idea was that the replacement of all three meals in the first week would lead to some kind of “reset”. In combination with concomitant blood glucose self-monitoring in the following weeks, an individualized diet should be gradually rebuilt. However, because of the similarity of the intervention design, we expected that the moderate diet regimen would lead to a significant improvement as well. We, therefore, included the comparison with a control group that received standard treatment.
The strengths of the present study comprise: (i) a relatively large number of patients studied per group who had poor controlled type 2 diabetes and a long type 2 diabetes duration; (ii) a longer study period compared to previous studies with formula diets (52 weeks vs. ≤26 weeks); as well as (iii) a randomized trial design with two intervention groups and one observational control group. Furthermore, the (iv) chosen real-world setting with a combination of formula diet, SMBG, and dietary education could be easily implemented into present health care programs. Likewise, another study with a real-world approach could demonstrate that even the partial use of a formula diet with one pack of formula diet instead of one of three daily low-caloric meals for 24 weeks was much more effective in reducing body weight and improving coronary risk factors than a conventional diet with a reduced energy intake in obese type 2 diabetic patients [41].
A limitation of our study is that we did not use food diaries to control for decreased calorie consumption or incorrect food compositions (e.g., the amount of carbohydrate in the diet, glycemic index, fat or protein intake) after the acute meal replacement phase from week 13 to week 52. However, the 52-week follow-up revealed that participants of both intervention groups showed no difference in maintaining the formula diet and following the dietary intervention until the study end (S-group 65%; M-group 63%). Also, more profound and quantitative diagnostics, such as isotope measurements, could have been done to control for food-related study compliance. On the other side, interventional studies with formula diets and similar results in a real-world setting [31] support our therapeutic approach in patients with poorly controlled type 2 diabetes.
Another factor, which should be considered, is the adjusted glucose-lowering medication dose in response to glycemic improvements due to the meal replacement intervention. It is conceivable that the impact of our formula diet on the HbA1c reduction is underestimated due to this adjustment. Another limitation of our real-world study is that the participants of the control group were not randomly assigned. In one of our previously published studies (NCT02066831), we found dramatic negative effects on HbA1c and dropout rate (26%) for the participants of the control group [16]. This approach, without a randomized control group with standard care, was also conducted in other benchmark studies for formula diet trials, like the Counterbalance Study (CS) [14] and the Counterpoint Study (CP) [15]. Both of the studies with small sample sizes (n = 11–29) reduced HbA1c (CS: −1.4% and CP: −1.1% to −0.6%) similar, as it was shown in our study after eight weeks of intervention. Furthermore, when comparing the present study results with findings from other landmark studies (DIRECT and TeLiPro study [17,21]), one can see that an assignment to the control group with standard care is accompanied with serious and disadvantageous effects, such as high dropout rates or even an increase in HbA1c. These findings support our approach and study design.
In sum, individualized low-carbohydrate diets can produce clinically-relevant reductions in HbA1c after 12 weeks of intervention. Furthermore, body weight, fasting blood glucose, quality of life, eating behavior, and other cardiometabolic risk factors improved, although not all of the parameters showed statistically significant improvements. Moreover, the initiation of a weight loss program with one week of full meal replacement (three meals per day) resulted in a clinically relevant long-term HbA1c reduction, when compared to an observational control group that had standard care. Our practicable and real-world setting-based approach led to relevant long-term improvements that were comparable with procedures of bariatric surgery without adverse events or negative side-effects. These results support the therapeutic concept of low-carbohydrate diets by formula diets in patients with poorly controlled type 2 diabetes.