Discussion
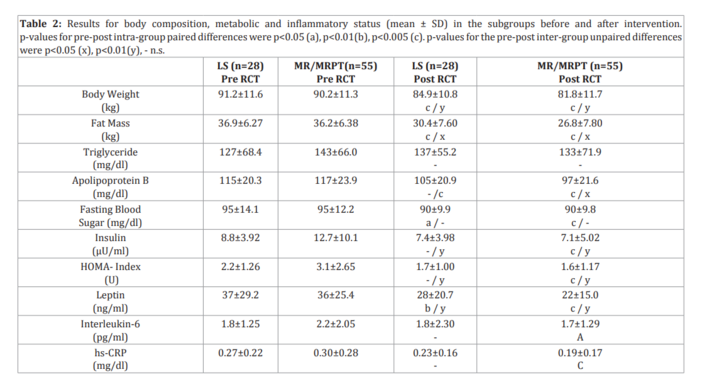
In this study, we compared the effects of different weightmanagement interventions, including therapeutic lifestyle changes and the use of a meal replacement product with or without supervised exercise training. Overall weight and fat loss were significantly greater in the meal replacement group. This group also demonstrated greater improvements in blood markers of metabolic health.
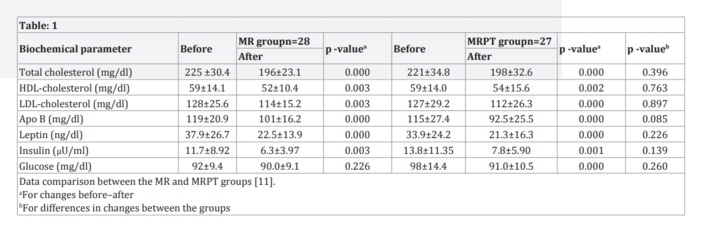
In 2003, for the first time, a team at Freiburg University published their findings regarding the positive effects of a soyyoghurt- honey-based meal replacement product (Almased®) on weight reduction and the regulation of insulin and leptin [11]. According to this randomized controlled trial, insulin and leptin levels decreased more in participants using the meal replacement compared to participants receiving lifestyle group counselling. In the current study, we conducted a secondary analysis of the first 24-weeks of intervention by merging the data of the MR and MRPT groups. The main trial findings were published in 2003 and indicated the beneficial effects of the meal replacement formula on reductions in leptin and insulin levels. These results were confirmed by our secondary analyses.
When the leptin results were adjusted for age, gender, baseline leptin level, body weight change, and intervention type (LS vs. MR/MRPT), the meal replacement approach clearly had an independent effect on plasma leptin levels and improved the effects on leptin reduction caused by weight loss. Therefore, the results suggest a relationship between protein intake and leptin regulation in the overweight adults examined. Several studies have demonstrated that an increase in the proportion of dietary protein from 15% to 30% of energy intake with a constant level of carbohydrate intake produces a sustained decrease in ad libitum energy intake, which may be mediated by increased central nervous system leptin sensitivity resulting in significant weight loss, while sparing muscle protein loss and enhancing glycaemic control [7, 11-12, 15-16]. Participants consuming a diet high in protein with a low glycaemic index continue to lose weight after the initial weight loss [13]. In fact, higher dietary protein intake was achieved by reducing carbohydrate intake, which adds further support to the concept that reducing glycaemic load (defined as dietary carbohydrate content (g) multiplied by glycaemic index) is important for controlling body weight in obese patients [17-19]. The satiating effect of protein and specific peptides (such as those found in soy protein isolates) may also contribute to the weight loss produced by low-carbohydrate diets [7, 20]. Moreover, weight loss interventions using meal replacement approaches together with dietary counselling and increased physical activity lead to substantial, favourable changes in both anthropometric and metabolic risk factors, while preserving lean muscle mass [12, 21].