Discussion
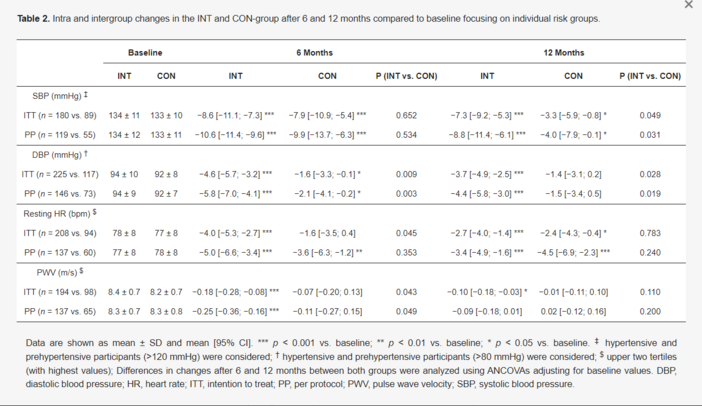
The results of this post-hoc analysis of the ACOORH trial indicate larger reductions in systolic and diastolic blood pressure as well as improvements in resting heart rate and pulse wave velocity after a 12-month intervention with a high-protein, low-glycemic, and moderate-caloric formula diet in high-risk individuals with overweight or obesity and accompanied cardiovascular risk factors compared to a low-intensity lifestyle intervention alone.
These findings are in line with other studies investigating the impact of weight loss due to different dietary and lifestyle approaches on cardiovascular risk factors in various populations [9,22,23]. For example, calorie restricted diets [22] or time-restricted eating approaches [23] have led to significant reductions in blood pressure and improvements of endothelial dysfunction. Furthermore, a recently published meta-analysis demonstrated comparable improvements in cardiovascular risk factors following weight loss intervention with diets of different macronutrient composition [9], pointing towards a more pronounced effect for improving systolic and diastolic blood pressure following a lower carbohydrate diet (e.g., Atkins diet). Moreover, adding a moderate-caloric restrictive diet to an aerobic exercise intervention demonstrated superior improvements in proximal aortic stiffness in older adults with obesity compared to exercise alone [24].
Although high-risk individuals of the INT group demonstrated moderate but clinically meaningful improvements in hemodynamic parameters, CON participants also showed clinically relevant changes. These small differences between both groups might have been derived from the dietary composition throughout the study. As recently published [25], both groups differed primarily in protein consumption which was embedded in a prescribed low-carbohydrate dietary lifestyle for both intervention groups. This explanation can be supported by a recently published meta-analysis showing the beneficial effects of higher compared to lower protein diets on cardiometabolic risk factors [26]. The mechanistic link behind this finding might have been derived from bioactive peptides that can inhibit the activity of the renin-angiotensin converting enzyme which is a key regulator for systemic hypertension [27].
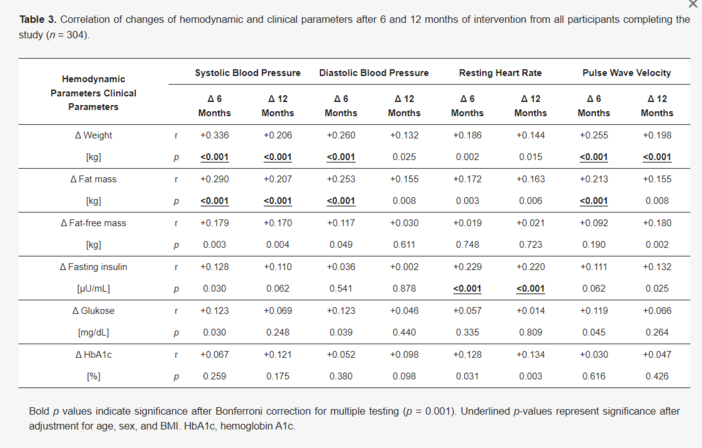
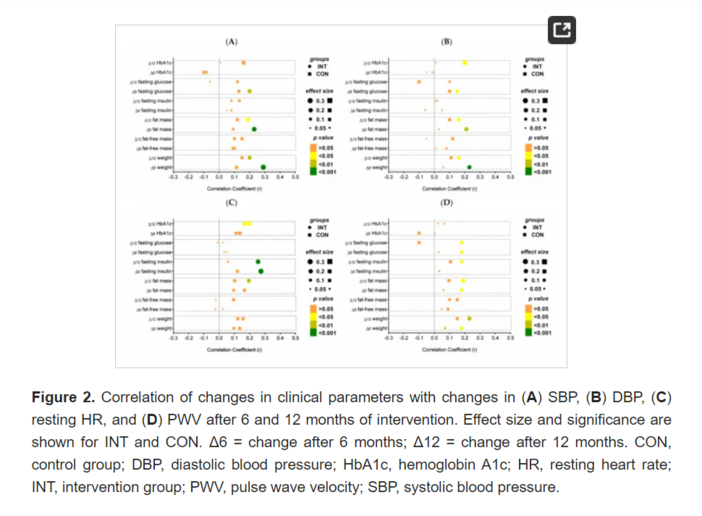
Findings of the correlation analyses of the whole cohort pointed towards physiological interrelationships between changes in fat mass and body weight with blood pressure and pulse wave velocity as well as interactions of fasting insulin and resting heart rate. These different associations may derive directly or indirectly from one pathophysiological mechanism of hyperinsulinemia or higher insulin levels leading to several further physiological maladaptive changes, for example: (1) sympathetic nervous system overactivity [28]; (2) enhanced renal sodium reabsorption [8]; (3) overstimulated renin-angiotensin-aldosterone system [8]; (4) proinflammatory processes and hypertrophy of vascular smooth muscle cells (or endothelial dysfunction and increased arterial stiffness) [28]; and finally (5) increases in body weight and obesity-associated hypertension [29]. One further key player in this context is insulin resistance, which in combination with hyperinsulinemia, may promote hypertension and atherogenesis. During insulin resistance, nitric oxide (NO) production is impaired while the supportive effect of insulin on calcium ion influx and vasoconstriction is still present [8]. Furthermore, adipokines—segregated by adipose tissue, impair the regulation of blood pressure, lipid and glucose metabolism [30] and changes in adipokine levels might have contributed to the improvement of hemodynamic parameters in the present study.
The strong positive correlation of resting HR with fasting insulin levels in the present study is in line with other studies demonstrating that insulin itself (even in different entities such as: fasting insulin, intact proinsulin, split proinsulin, or acute insulin response [31]) can influence the cardiac autonomic nervous system by reducing parasympathetic function and potentiating sympathetic drive in patients with [32] and without diabetes [33].
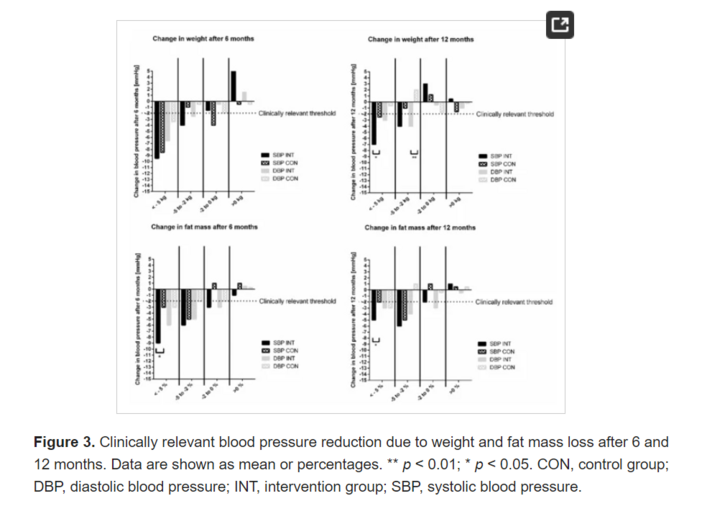
When discussing the sustainability of the intervention effects, changes of SBP and DBP, which were primarily associated with changes in weight and/or fat mass, seem to be more long-lasting than resting HR and PWV. Resting HR was, especially, probably more related to short-term physiological changes of insulin, which have been shown to be present in particular during the intensive phase of the study [15]. The primary intervention was within the first 6 months (intensive phase) and the last 6 months were characterized as a maintain phase (less intensive phase). The decline in treatment intensity maybe led to this immediate physiological adaption of insulin, also influencing negatively the sympathetic nervous system while weight loss and/or fat mass reduction was more sustainable, and, therefore, SBP and DBP were significantly different between both groups even after 12 months of intervention. The landmark studies of DiRECT [11] and DIADEM-1 [34] have already shown in patients with type 2 diabetes that, in particular, weight-loss mediates the reduction of blood pressure.
Frequency of antihypertensive medication use was not affected by the intervention in either group. One possible explanation for these findings is, that, on the one hand, compared to very-low or low-caloric diet interventions with partial abandonment of antihypertensive medication [11,35], the present study applied a moderate-caloric diet (≈1300–1500 kcal per day) approach, with the aim of increasing study and treatment adherence and reducing the risk for adverse outcomes in the long-term [36]. On the other hand, reduction of antihypertensive medication was not targeted and not all participants were hypertensive or prehypertensive with an accompanying antihypertensive therapy.
The strengths of the present post-hoc analysis comprise a large sample size of only high-risk participants with overweight or obesity and at least one additional co-morbidity of the metabolic syndrome, the international, multicenter and randomized controlled setting of the study, and a relatively long study period over 12 months. Although study participants were comprehensively characterized, information about smoking status as well as kidney-related data (e.g., creatinine levels or urinary sodium excretion) were not included, which should be considered when interpreting the data. A recently published meta-analysis demonstrated that a reduction in dietary sodium can have beneficial effects on blood pressure levels in different populations [37]. Moreover, it has been shown that cardiorespiratory fitness also has a marked impact on the autonomic nervous system in patients with and without diabetes [38,39]. In particular, parasympathetic drive increases with enhancing cardiorespiratory fitness. This aspect was not part of the investigation and should be considered when interpreting the data. Further limitations of the present study include that there was no constant diet monitoring. Based on the issue of biased dietary records with systematic errors, we chose to omit monitoring the participants’ diets [40]. However, 4-day diet diaries prior to each study visit were required from all participants to support the lifestyle counseling. Furthermore, although sophisticated imputation methods for missing values are currently indicated, we consciously chose the LOCF procedure for a more conservative statistical approach to prevent overestimating the present results of this post-hoc analysis. Another aspect which needs to be considered, especially when discussing the changes to the resting HR data, is that there is a possibility of an unconscious habituation towards the examination procedure which might have influenced the measurements. However, randomization into one of the two groups should have abolished any potential habituation effect, particularly because baseline characteristics of both groups were not different. On the other hand, the strong interrelation between fasting insulin and resting HR at any time point, particularly for the INT group, indicates rather a physiological adaption of resting HR due to the intervention.